After dropping out of school for a year, William recently returned to high school at his mother's request. As a 17-year-old taking freshman courses, he was unmotivated and moody, and he felt out of place. Yet his mother was determined that her son finish high school even though he was far behind.
A teacher suggested that William meet with a staff member at the school's Youth and Family Center, one of nine such primary care and counseling facilities that provide support services to Dallas students. William went to a counselor and revealed what else had been weighing on him: He had seen a gang member kill his older brother at their home. He desperately missed his father, who was in prison.
The Youth and Family Center staff offered counseling to the whole family—William, his mother, and his younger brother. William also began to take GED classes so that he could earn his diploma in a more age-appropriate manner.
Frances, a 3rd grader, and her family were also referred to the Youth and Family Center. They arrived in crisis, in need of food, shelter, and assistance in paying bills. The case manager helped them find housing and obtain food and clothing, while a therapist provided family counseling.
Two other students, David and Alicia, visited the center for medical problems. David's mother brought him because his left eye was red and swollen. The medical team diagnosed an infection and sent him home with a prescription for antibiotics. Alicia's problem turned out to be more complex. A 16-year-old high school junior, she complained of an earache, but as she talked with a nurse practitioner, she revealed that her boyfriend had hit her on the head the previous evening. Recognizing that Alicia was in an abusive relationship and that she was unsure how to change it, the nurse practitioner referred her for counseling at the center.
A Holistic Approach
Of the 154,000 students in Dallas public schools, 67 percent meet poverty guidelines, and 39 percent are considered at risk for dropping out of school. The number of at-risk students increases from elementary (33 percent) to middle (40 percent) to high school (47 percent). For these students, many factors stand in the way of academic success—poor nutrition, violence, substance abuse, inadequate health care, mental health problems, and minimal parental academic support.
Like other proponents of school-linked services, district officials knew there is a direct connection between students' social, emotional, and physical health and their academic performance. Yet despite the great need for assistance for disadvantaged students and their families, support services in Dallas schools have historically been fragmented and uncoordinated, limited to specific areas of the city, and offered at inconvenient hours.
In coming up with a solution, district officials felt that schools would be natural places to meet students' nonacademic needs. They are longstanding community institutions; they are accessible; and they lack the stigma so often attached to social service agencies (Koppich and Kirst 1993, Wagner and Gomby 1996). Officials also wanted to approach children's physical and emotional well-being holistically, through family-focused, preventive services.
In the summer of 1995, the district formed a partnership with the Parkland Health and Hospital System's Community Oriented Primary Care Division and the Dallas Mental Health-Mental Retardation Agency's Child and Adolescent Services Division. The result was the opening in the fall of 1995 of nine Youth and Family Centers, each one located on or near a school campus. The Parkland hospital system provides staff and medical supplies, the Dallas agency furnishes staff for intensive mental health services, and the school district hires staff members to coordinate all the services, using federal Title XI funds to cover coordination and administration costs. The school district also pays for occupancy costs.
The services offered are designed to promote academic success, resiliency, and self-sufficiency for students and families. In addition to the core services—medical care, intensive mental health counseling, and general counseling—the center customizes assistance for families in the surrounding community. All students and families have access to 24-hour emergency and crisis intervention. And the center staff encourages parents to participate fully in the treatment of their children and other family members (see fig. 1).
Figure 1—Dallas Youth and Family Center Services
Linking Schools with Youth and Family Centers - table
Physical Health | Mental Health | Support (varies by site) |
|---|---|---|
| Health maintainance exams | Psychiatric evaluations | Life skills courses |
| Urgent care | Family therapy | ESL classes |
| Immunizations | Student therapy | GED classes |
| Sports physicals | Group therapy | Citizenship classes |
| Medication | Student support groups | Art classes |
| Nutrition counseling | Family support groups | After-school activities |
| Labwork | Parent support groups | Recreational activities |
| Chronic disease management | Parent education classes | |
| Student social skills classes | ||
| Medication | ||
| Classroom behavior plans |
Promising Results
In the first year of the program, more than 3,400 students used the services of the centers. Managers logged a total of 3,686 physical health visits, 2,677 mental health visits, and 1,485 support service visits.
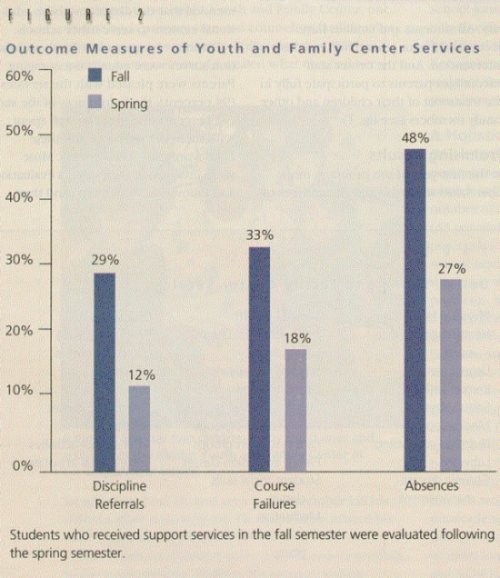
As Figure 2 shows, the effect of the program, which began in the fall, was promising. More than half the students with behavior problems noticeably improved from fall to spring. Similarly, nearly half of those referred with attendance and academic problems showed notable progress by the spring. In all cases, the outcomes were statistically significant.
Figure 2. Outcomes Measures of Youth and Family Center Services
The questionnaire distributed to principals after the first year reflected an equally positive outcome. Virtually all the principals believed the centers provided quality services (98 percent), had a positive reputation (93 percent), and were valuable to their students (96 percent). All the principals recommended that the district establish additional centers to serve other schools.
Parents' responses to a family satisfaction survey were equally encouraging. Parents were pleased with the services (94 percent), the helpfulness of the staff (97 percent), the time the staff spent with them (91 percent), and their child's progress (86 percent). Most were involved in their child's evaluation and follow-up (94 percent) and they indicated that they would return to the center if they had the same problem again (92 percent).
Students' performance on standardized tests was mixed. More students passed the Texas Assessment of Academic Skills, but their scores on the reading and math segments of the Iowa Test of Basic Skills were lower. We hadn't expected an upsurge in scores because most centers were not fully operational until the end of November. Rather, we intend to use the scores as baseline data for future analysis (Bush 1996).
Critical Lessons
- Melding the services of three large bureaucracies to provide health and support services in a comprehensive, integrated way requires a major effort and considerable determination. Cross-training is necessary to familiarize staff members with the services of each project partner as well as the common terminology, procedures, and paperwork requirements. The training ensures smoother service delivery to families.
- Governing coordinated services is demanding and time-consuming. Center staff members spend many hours planning, creating policies, and handling site-level details. Project partners handle governance issues through monthly meetings and memorandums of agreement. A subcommittee of partner staff members meets weekly to tend to daily needs. In the time available, members try to strike a balance between making decisions about policy issues and center-level details.
- Strong center managers who know the community and who work well in a school setting are critical. Managers must be able to work effectively with many people—principals and other school personnel, clients, and community members. They need to understand how the school system and individual campuses work. They also must be comfortable and visible in the schools and in the community to assemble resources and match them to families in need.
- No one set of services works at all sites. Student and family needs vary in different communities. Although all centers provide physical and mental health services, staff members tailor other services to the needs of their clients.
- In overcrowded schools, it's difficult to find sufficient space to allow for the privacy, comfort, and efficient use of time of students and families. Creativity and flexibility are essential. Close cooperation with the school staff has allowed the use of teachers' lounges, counselors' offices, cafeterias, and classrooms for group or individual sessions and instructional activities after regular school hours. On occasion, the center staff has used such community facilities as churches and the YMCA. At certain sites, freestanding buildings have proved useful, enabling the centers to operate in the evenings and on nonschool days.
- Providers must ensure confidentiality as they share conceivably stigmatizing information about children and family members. The project partners have developed policies that enable them to share information but safeguard it from access by others.
- Federal categorical funding (Title XI school funds) covers only basic costs like the coordination of services and case management. For direct services, the centers depend on other agencies.
- Evaluation is an integral part of the planning and management process. Feedback throughout the year enables the staff to focus on problems, modify staff training, and plan for the future. Both outcome and process information is important in assessing the program's overall effectiveness and in documenting what the centers do (Davis 1995, Shaw 1995, Garnett and Gould 1996). Trust between the evaluator and project staff is crucial.
As we noted earlier, our evaluation results were encouraging. We have been able to help students like William, Frances, David, and Alicia, whose plights exemplify the problems that students in our school district face. David's eye quickly healed, but we continue to follow the progress of the other children. Our hope is that by resolving their nonacademic problems, we will give them a much better chance of succeeding in school.